Identifying lipid deposits that put patients at higher risk of major adverse cardiovascular events enables early clinical treatment of coronary disease.
NICHOLAS C. GIGLIO, SAMANTHA FARROW, KAVYA SREERAM, AND STEPHANIE GRAINGER, INFRAREDX, A NIPRO COMPANY
Lipoproteins carry cholesterol through the closed-looped vascular hematological highway of the human body. This cholesterol can embed itself into the artery walls at varying rates, depending on a multitude of factors, such as anatomical influences or genetic predispositions. Cholesterol vascular wall infiltration triggers the body’s immune response to multiply collagen and muscle cells in these specific regions of vascular tissue, forming a fibrous cap over the lipid deposit (Figure 1). A progression of optical technologies has been put to work to capture these deposits — most recently, near-infrared spectroscopy (NIRS), in conjunction with other modalities.
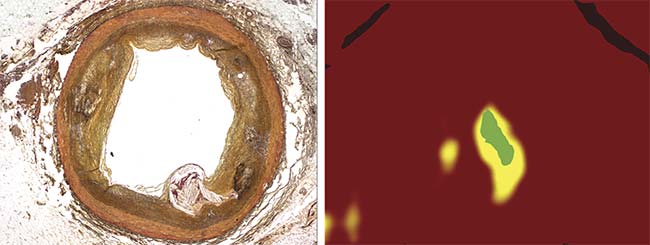
A chemogram (right) showing lipid composition (yellow). A concept art display of low collagen areas (green) corresponds to the Movat’s Pentachrome stained histology slide (left). Note the well-defined and bulging lipid core with the very thin region of fibrous cap overlying it. Courtesy of Infraredx.
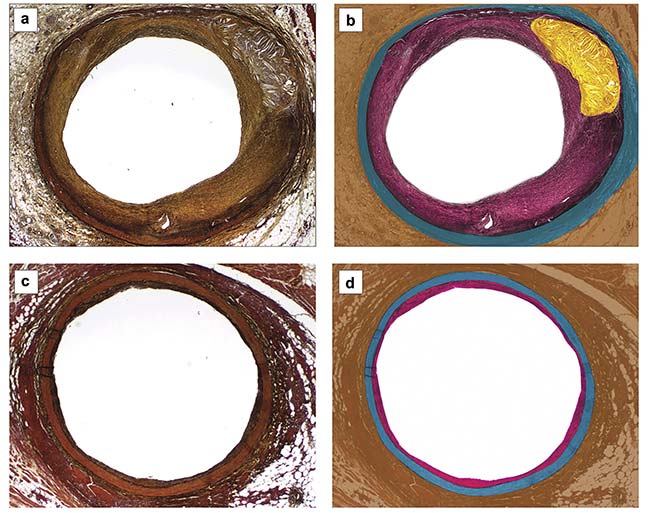
Figure 1. Movat’s Pentachrome stained slides of diseased (a) and healthy (c) coronary arteries. The corresponding representations show the layers: tunica externa (brown), tunica media (blue), tunica intima (pink), and lipid (yellow) (b, d). Note the increased thickness of the tunica intima and lipid core, only present in the diseased sample. Courtesy of Infraredx.
When the intralipid core stress exceeds the material strength of the fibrous cap, the plaque can rupture. These ruptures are proven to cause major adverse cardiovascular events in the form of acute coronary syndromes and sudden cardiac death. Histopathological studies have shown that lipid core plaque burden within an artery wall is one of the main compositional characteristics used to predict a coronary event. The ability to directly measure the amount of lipid core deposited within a vascular wall cross section allows for the prediction of the likelihood of a coronary event. Gold standard cardiac catheterization laboratory imaging techniques — such as angiography, optical coherence tomography (OCT), and standalone intravascular ultrasound (IVUS) — provide useful structural information but cannot distinguish underlying pathological differences within a plaque burden. Claims of OCT-based lipid detection systems are based on external observer analysis and have demonstrated at least a 20% false-positive rate1.
A more recently developed intravascular imaging method uses near-infrared spectroscopy as an automated diagnostic tool. NIRS and IVUS have been successfully validated with histology and cleared by the U.S. Food and Drug Administration (FDA) to detect lipid core plaque in coronary arteries and identify patients and plaques at a higher risk of major adverse cardiovascular events.
The utility of NIRS
Intravascular NIRS is the measurement of spectra between 1000 and 2000 nm produced by laser interactions with nonhomogeneous biological tissue. The nonhomogeneous layers of propagation through a healthy artery are made up of blood, mainly containing red blood cells, white blood cells, platelets, and plasma; tunica intima, mainly consisting of endothelial cells; tunica media, mainly consisting of smooth muscle cells and elastin fibers; and the tunica externa, mainly consisting of collagen fibers. As discussed, in a nonhealthy artery, a thicker layer of connective tissue is present in the intima layer, as well as an additional layer of lipid core plaque. When photons interact with these varying layers, a unique photon signature is generated that is dependent on the morphology and thickness of the layers.
Intravascular photon interaction induces three main events: reflection, absorption, and scattering. Both specular and diffuse reflections primarily occur at boundary conditions that can be quantified by Fresnel equations governed by the change in the index of refraction. However, since NIRS is not depth resolved and is therefore determining bulk material within the entire depth of a cross section, the primary focus is on the understanding of absorption and scattering events.
Absorption is the complete transfer of photon energy to the biological material, such as tissue, which generally transfers energy into the molecular vibrations of the tissue. The absorption event is only highly efficient at very specific wavelengths. This process can be visualized using classical physics such as the Lorentz oscillator model, which describes the effects that electromagnetic waves have on material bodies. The most efficient wavelength absorptions occur at multiple resonant frequencies. However, unlike the Lorentz oscillator model, there is no defined lattice structure in biological tissues, and, therefore, the absorption spectrum is determined experimentally as a spatial frequency that is unique to each biomaterial2.
Nonabsorbent intravascular photon interactions can result in the reradiation of light at varying angles and are distributed from the event point as a function of the anisotropic factors in the biological material. This interaction is determined by the Henyey-Greenstein phase function and referred to as scattered light. The total amount of scattering that occurs in the material per unit path length is predicted by the wavelength-dependent spatial frequency occurrence of a scattering event2. The optical penetration depth of light through biological material is represented by an exponential decay, which is directly related to the scattering and absorption events, and occurs when the initial light intensity is reduced to 37% of its initial value.
Performing reflective spectroscopy for vascular embedded lipid detection without blood clearing invokes the need for wavelengths to be chosen to optimize for low absorbance in blood, collagen, and stenting material, and for higher absorbance in cholesterol. Near-infrared wavelengths are used for intravascular spectroscopy due to their ideal optical penetration depth, with high absorption in cholesterol and low absorption in blood (Figure 2)3,4.
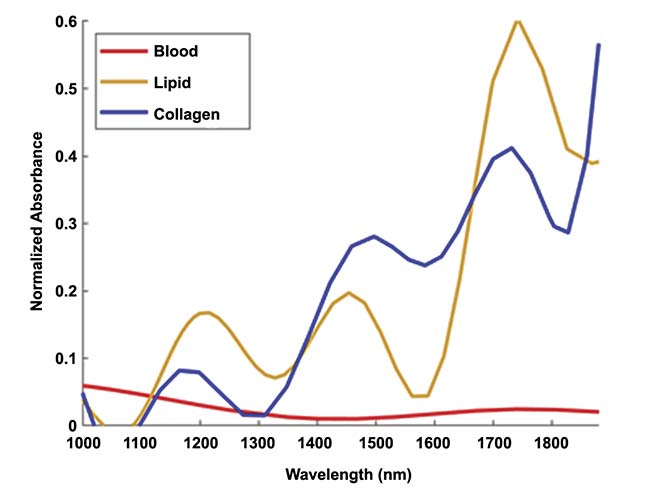
Figure 2. Near-infrared spectra of cholesterol, collagen, and blood. Adapted with permission from
References 3 and 4.
An ultrafast swept-source system ranging within a cholesterol absorption peak is used for intravascular NIRS. The ultrafast sweeping source provides measurements without interference from cardiovascular motion. The output power of the system will vary depending on individual total system loss; however, successful spectroscopy is achieved when sufficiently high laser power is applied to collect a back-scattered signal. This creates a discernible signal-to-noise ratio. The laser power upper limit prevents photothermal effects on the vascular tissue. To guarantee these laser parameters, the laser signal is closely monitored with a reference channel for a known laser power. This reference channel is also used in calculating the final resulting lipid concentration.
System components
An example of a system working for this purpose would be the Dualpro IVUS+NIRS imaging catheter, which consists of two fiber optics and a single ultrasound transducer, bundled together within a 3.2-French catheter. The catheter has both rotational and linear actuation inside of the artery to give a full 360° image of a 150-mm artery length with speed acquisition between 0.5 and 2.0 mm/s.
NIRS alone does not provide depth resolution or structural information; therefore, ultrasound is a complementary feature within such a catheter. IVUS can quantify the lumen dimensions and identify the structural characteristics of the vessel wall, allowing the user to accurately select a properly sized stent. Co-registered NIRS and IVUS can produce a structural map from lipid detection. The light scatters deep within the artery and back to the catheter, where it is collected by a larger mirror and coupled into a multimode fiber optic (Figure 3).
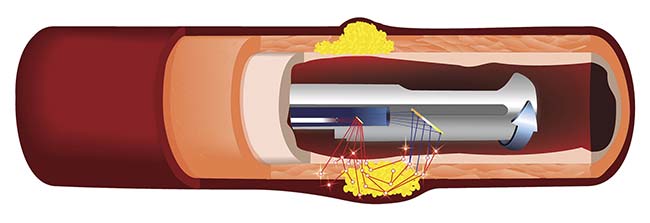
Figure 3. A schematic of an IVUS+NIRS catheter showing light delivered from a fiber (red), scattering and absorption events in the blood and tissue layers (white stars), and light collected into a fiber (blue). At each scattering or absorbing event, the light interacts with its surrounding materials — blood (red), artery wall (pink), and lipid (yellow) — and delivers the information back through the catheter to a detector. Courtesy of Infraredx.
A combined system, when the signal is detected by a photodiode, can be processed using mathematical models derived from chemometrics, an analytical technique that applies mathematical and statistical modeling to derive signal composition from complex biological mixtures. Automated information can then be viewed via a console user interface that generates both an IVUS and NIRS image in both a longitudinal and transverse cross section (Figure 4).
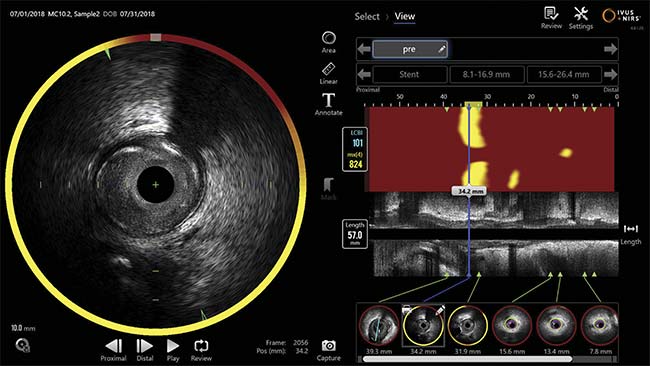
Figure 4. The Makoto console user interface shows the red-yellow chemogram (upper right) and the grayscale intravascular ultrasound (IVUS) longitudinal image (middle right). The chemogram shows lipid detected (yellow areas). The cross-sectional image contains the chemogram halo co-registered to the IVUS transverse image (left). Courtesy of Infraredx.
The NIRS image is called a chemogram, which is a false-color, two-dimensional map of the lipid core plaque probability distribution across the lumen surface of the scanned artery. The chemogram pixels range from red (for low probability) to yellow (for high probability) of the lipid core plaque. The automated algorithm also generates a single metric that quantifies the maximum angular extent of lipid core plaque — known as the maximum lipid core plaque burden index — within a 4-mm-long cross section from each scan. This information has proved itself to be useful in the clinic for both stenting and other treatment decisions.
Current clinical impact
Clinical studies have shown that intravascular NIRS is capable of imaging both nonobstructive and obstructive coronary arteries and can identify both patients and nonculprit plaques that are at high risk for future events.
A lipid-rich plaque study aimed to evaluate the correlation between the presence of nonintervened, nonflow-limiting, lipid-rich plaque and the future development of major adverse cardiovascular events over a span of two years. The results demonstrated that, when calculating an NIRS-based maximum lipid core plaque burden index value greater than 400, a patient is at an 89% higher risk of an event, and an individual coronary segment is at a 322% higher risk5.
NIRS was also used to study vulnerable plaques in patients undergoing percutaneous coronary intervention in both the PROSPECT II and PROSPECT ABSORB trials. In PROSPECT II, NIRS and IVUS improved the ability to identify the plaques that were at the highest risk of future cardiovascular events. In PROSPECT ABSORB, a subset of randomized patients was the first potential patient cohort to have the newly identified vulnerable plaques prospectively treated with a bioresorbable vascular scaffold to increase the minimum lumen area and stabilize them.
NIRS has the ability to see through stented sections of an artery and is commonly used to guide clinical decision-making regarding stenting a subsection of vascular structure. Clinical studies evaluating the accuracy of stent lengths using NIRS metrics showed that in 16% of the cases, the lipid core plaque extended beyond the treatment margins as determined by gold standard angiography6. Determining stent placement within the vascular structure is critical, because underestimations in stenting length can lead to nonstented, high-risk lipid core plaque subsections that can be directly correlated with cardiovascular events. Therefore, NIRS imaging aids the determination of the margins of treatment, in both length and placement of stents.
Recent studies have focused on the use of NIRS to guide drug treatments. The PACMAN-AMI and YELLOW III trials used NIRS to quantify the decrease in the cholesterol content of atherosclerotic plaques following treatment with a newer class of drugs, called PCSK9 inhibitors, that work in statin-resistant patients. The results show that NIRS provides a metric to quantify the effects of drugs in clinical trials and that it lays the groundwork for the future use of intravascular NIRS to quantify the effects of additional drug treatments.
Future NIRS applications
Significant advancements in intravascular NIRS technology are already underway, with a primary focus on the ability to use NIRS technology to detect the structural integrity of the fibrous cap overlaying a lipid deposit. The thickness of the lipid core plaque cap has been accepted as a metric to indicate the probability of plaque rupture, but new findings indicate that the collagen content of the fibrous cap is an important factor in assessing the risk of major adverse cardiovascular events. Studies have shown a poor correlation between cap thickness and cap collagen composition, which indicates that collagen composition provides information that is unrelated to cap thickness7.
Additionally, within samples of equal cap thickness, the collagen composition can vary widely and possibly indicate a different risk of a future cardiac event. Using a trained algorithm, intravascular NIRS technology can be used to identify collagen content in addition to lipid core plaque presence. Initial testing was quantified via a pixel-counting method using linearly polarized picrosirius red-stained histology slides as the truth reference for model building. The generated model can predict structurally weak caps based on the given training data. This model can be further applied to a multitude of available data sets to explore predicted weak caps by collagen content, as well as the resulting outcomes in patients.
Since intravascular NIRS technology can be used to identify both lipid core plaque and collagen composition simultaneously, it can potentially provide greater automated clinical guidance for identifying plaques that are at the highest risk of causing future adverse cardiovascular events (see image on page 38). In addition to lipid core plaque and collagen content, intravascular NIRS contains a host of untapped potential that can be visualized by the plethora of unexplored applications. Future work will focus on expanding NIRS characterization of different targets, as well as the potential for combining a multitude of existing intravascular technologies, either structural or physiologic. The physical addition of other imaging technologies, such as optical coherence tomography, or the virtual addition of AI-based methods to improve image interpretation activities are both possible directions to improve upon the compositional plaque characterization that NIRS already provides.
Meet the authors
Nicholas C. Giglio, Ph.D., earned a bachelor’s degree in physics and mathematics from the University of North Carolina at Charlotte (UNCC), a master’s degree in biomedical engineering from the University of Rochester, and a doctorate in optical science and engineering from UNCC. He is currently working as senior scientist at Infraredx, developing novel optical medical applications; email: [email protected].
Samantha Farrow obtained a bachelor’s degree in biomedical engineering from Wentworth Institute of Technology in Boston. In 2017, she joined Infraredx, where she currently works as senior biomedical engineer with the research group, focusing on phantom development for NIRS system improvement; email: [email protected].
Kavya Sreeram earned her bachelor’s degree in bioengineering from Temple University and a master’s degree in biomedical engineering from New York University, where she wrote her thesis on applying machine learning techniques to optical data. She now focuses on model and algorithm development as senior biomedical engineer at Infraredx; email: [email protected].
Stephanie Grainger, Ph.D., earned a bachelor’s degree in chemical engineering from the University of New Hampshire, and a master’s degree and a doctorate in biomedical engineering from the University of Michigan. She is currently leading the research group at Infraredx, where the team develops refined and new applications of NIRS; email: [email protected].
Acknowledgments
The authors thank Gina Miller for her assistance in image design and Stephen T. Sum for his mentorship.
References
1. E.M.J. Hartman et al. (2022). Wall shear stress-related plaque growth of lipid-rich plaques in human coronary arteries: near-infrared spectroscopy and optical coherence tomography study. Cardiovasc Research, cvac178, pp. 1-9, www.doi.org/10.1093/cvr/cvac178.
2. N.C. Giglio. (2022). Infrared laser fusion and bisection of blood vessels with real-time optical diagnostics feedback. Ph.D. dissertation. University of North Carolina.
3. J.T. Kuenstner and K.H. Norris. (1994). Spectrophotometry of human hemoglobin
in the near infrared region from 1000 to 2500 nm. J Near Infrared Spectrosc, Vol. 2, No. 1, p. 59.
4. S.T. Sum et al. (2009). Near-infrared spectroscopy for the detection of lipid core coronary plaques. Curr Cardiovasc Imaging Rep, Vol. 2, No. 4, pp. 307-315.
5. R. Waksman et al. (2019). Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: a prospective, cohort study. Lancet, Vol. 394, pp. 1629-1637.
6. S.R. Dixon et al. (2011). Analysis of target lesion length before coronary artery stenting using angiography and near-infrared spectroscopy versus angiography along. Am J Cardiol, Vol. 109, pp. 60-66.
7. J. Su et al. (2016). Depleted collagen as a possible measure of cap weakness in human coronary autopsy specimens. J Am Coll Cardiol, Vol. 67, No. 13, p. 590.