Scientists are using photonic technology to enable fluorescence, absorption, and other factors to display the presence of infection in the blood.
 When a person develops Lyme disease from a tick bite, identifying the tiny culprit can be challenging. The insect itself is difficult to see in the grass or forested area it comes from before burrowing into the person’s skin. The symptoms of the disease, which afflicts hundreds of thousands each year, however, become clear to those stricken — ranging from fever and arthritis to damage to the nervous system. Fortunately, new testing modalities made possible by optical technology may soon enable clinicians to see changes far smaller than insects in grass — to peer inside a person’s system and identify disease antibodies within his or her blood, and expedite the process of reaching a diagnosis that historically may have taken weeks after infection.
When a person develops Lyme disease from a tick bite, identifying the tiny culprit can be challenging. The insect itself is difficult to see in the grass or forested area it comes from before burrowing into the person’s skin. The symptoms of the disease, which afflicts hundreds of thousands each year, however, become clear to those stricken — ranging from fever and arthritis to damage to the nervous system. Fortunately, new testing modalities made possible by optical technology may soon enable clinicians to see changes far smaller than insects in grass — to peer inside a person’s system and identify disease antibodies within his or her blood, and expedite the process of reaching a diagnosis that historically may have taken weeks after infection.
As with any illness, the earlier a proper diagnosis is provided, the sooner effective treatment can begin. Often, in the case of Lyme disease, antibiotics can alleviate symptoms, though antibodies can remain in the system for years after recovery. A recent infection, however, may take time to diagnose. Researchers have set to work to adapt simple testing strips and wearable technology to facilitate fluorescence and absorption and other phenomena in blood serum samples — along with optical modalities to measure blood oxygen levels — that can reveal the origin of a condition (whether Lyme or another ailment), sooner rather than later.
Lyme disease is primarily caused by the bacteria species known as Borrelia burgdorferi, as well as by Borrelia mayonii. The disease is spread to humans through blacklegged ticks, which have also generally infected the local deer population. According to the Centers for Disease Control and Prevention (CDC), some estimates place the annual infection rate at over 450,000 people in the U.S., with the majority of cases concentrated around the Great Lakes region and the Northeast, extending into Canada. But in 2018, the most recent year for which statistical information is available from the CDC, an incidence rate of at least 10 confirmed cases per 100,000 people was reported over a wide geographical area that included counties in states in the Northeast, the Great Lakes region, and the Southeast: Connecticut, Delaware, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont, Virginia, West Virginia, Washington, D.C., and Wisconsin.
One of the most common early symptoms of Lyme disease is erythema migrans (rash), which appears in the majority of those infected1. In its early stages, the disease produces fevers and myalgia, and, if untreated, it can produce skin lesions, meningitis, or carditis. Large-joint arthritis and neuropathy may appear in the latter stages, often lingering after treatment (Figure 1).
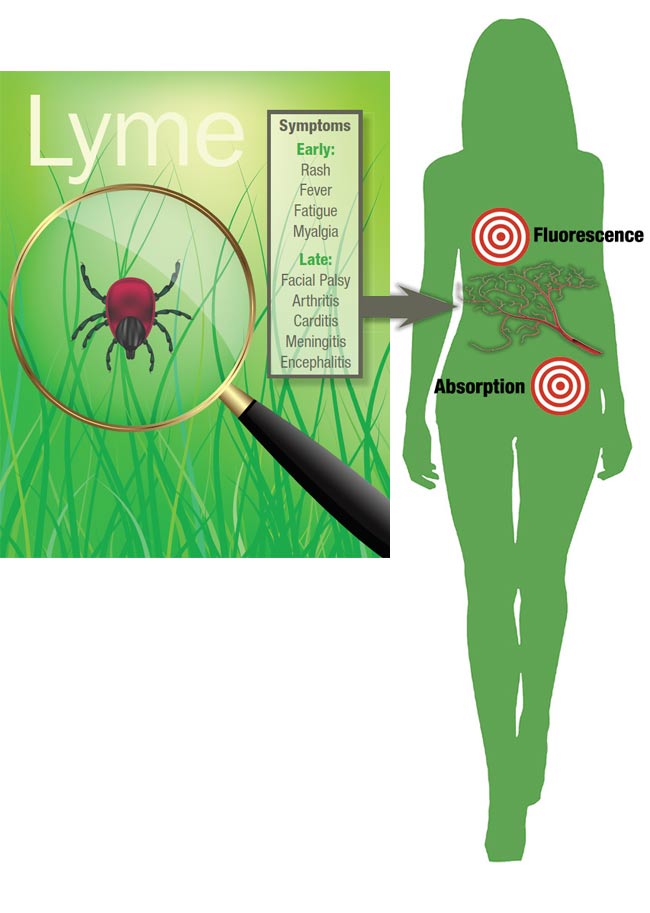
Figure 1. An illustrative interpretation of Lyme disease after contraction from a tick. Courtesy of iStock.com/Artsergei (magnifying glass and tick); iStock.com/msan10 (silhouette); iStock.com/Andrey Prokhorov (blood vessels); and iStock.com/FotografiaBasica (bull’s-eyes).
Limits of current testing
In the U.S., the CDC’s recommended laboratory test for the illness consists of a two-tiered analysis. The first is either an enzyme-linked immunoassay, wherein an enzyme-bound antibody produces a color reaction when exposed to an antigen (often present on a microplate), or an immunofluorescence assay, wherein virus cells are grown on glass and an antibody (linked with a fluorescent agent) is introduced, making the infection visible under a microscope. The second step is reflexive immunoblotting, commonly called Western blotting, wherein the proteins in a sample are separated and placed (blotted) on a membrane, then incubated with an antibody to provoke a reaction. When combined with a reporter enzyme that produces light, the reaction can indicate a positive result under the microscope. This standard test costs $200.
Many researchers currently engaged in adapting optical technologies to the diagnosis of Lyme disease point to the low sensitivity of the two-tiered test, particularly in the early stages of the illness, as a rationale for their work. Some analyses put the sensitivity in the range of 30% to 40%. This not only explains the often reported false negative results, but also raises the specter of patients not seeking further tests until symptoms become severe — such as when they spread to the nervous system — resulting in protracted treatment and recovery. Some positive tests even result from antibodies that have remained in the system for years after a prior infection and treatment1.
Blood-based Lyme testing can be divided into two categories: direct and indirect. The former identifies the disease-causing bacteria and the latter highlights antibodies to the disease, just as in the standard two-tiered test. Direct-detection testing methods include culture and polymerase chain reaction (both of which can be problematic because the bacteria leave the system quickly), and antigen detection, which identifies proteins from the bacteria.
Looking at Lyme
A team composed of researchers from UCLA and New York Medical College recently developed a point-of-care serodiagnostic test for Lyme disease, in which gold nanoparticles bind with the inherent antibodies present in blood serum. The colorimetric response, or the degree of absorption of particular wavelengths of light that indicates the presence of certain elements, was measured with a paper-based vertical flow assay. The work was performed after the group was approached by the Steven & Alexandra Cohen Foundation, a nonprofit sponsor of Lyme research, to develop a diagnostic alternative to currently accepted practice.
In the study, the group described the assay as a stack of paper layers that allow for the detection of an array of Lyme-specific antibodies at multiple locations on one sensing membrane contained within the assay cassette. The assay is performed using the cassette, and it is then imaged with a mobile phone-compatible device that reads the colorimetric signals2.
The capability is then enhanced via an algorithm that, by utilizing a subset of a data based on the visible reactions, can help to establish a diagnosis. This machine learning approach was trained using 50 human serum samples — 25 early Lyme disease samples and 25 samples from a control group, gathered by the Lyme Disease Biobank.
“The gold nanoparticles, which are well established in lateral flow assays, serve as a signal generator,” said Zachary Ballard, a postdoctoral researcher who earned his doctorate while working in the lab of Aydogan Ozcan at UCLA. “We used those means to measure multiple immunoreactions in our samples. In the body, Immunoglobulin M (IgM) anti-bodies are produced quickly in response to a disease or virus, and Immunoglobulin G (IgG) antibodies are produced more slowly, generally providing a longer-term defense against infection.”
Ballard said the researchers picked out assays for seven Borrelia-specific antigens and a synthetic peptide (amino acid) in the multiplexed assay and found that in both sensitivity and specificity, the results hovered around 90% in effectiveness. This held true regardless of the geographic area where the sample came from.
He said the UCLA team has launched a startup to commercialize the use of the materials for Lyme disease detection. He anticipated a two- to three-year timeline to reach market, during which both FDA clearance and a Clinical Laboratory Improvement Amendment waiver would be sought.
“With this relatively simple setup, we hope to reach areas where people might not have easy access to health care, such as rural areas that would be at risk for Lyme disease,” Ballard said. “We wanted to make this as low cost as possible.”
A long-standing collaboration between researchers at the State University of New York (SUNY) Polytechnic Institute in Albany, N.Y., and Ciencia Inc. in East Hartford, Conn., has created detection chips that are analyzed using Ciencia’s proprietary plasmonic fluorescence instrument. Now the team hopes it is getting closer to approval for early Lyme disease diagnosis (Figure 2).
Figure 2. An illuminated biochip, based on grating-coupled fluorescent plasmonics (GC-FP) technology, undergoing analysis. The biochip can be scored using an algorithm to diagnose Lyme disease and
potentially other conditions as well. Courtesy of Nathaniel Cady.
“We had interest in the molecular analysis of Lyme disease and the detection of bacteria,” said Nathaniel Cady, an Empire Innovation Professor in the SUNY Polytechnic College of Nanoscale Science and Engineering. “And we evolved from being the supplier of chips to Ciencia, to working on biosensing assays for that purpose.”
The scientists and researchers involved in the project knew that the antibodies IgM and IgG were present in people in the early stages of Lyme disease, but the antibodies can also be identified, to some degree, in patients who have been treated.
The researchers’ published study defines their approach as a grating-coupled fluorescent plasmonics (GC-FP) technology, which enables the multiplexed biomarkers screening of blood serum on a biochip that later can be algorithmically scored for diagnostic purposes (Figure 3). This method depends upon surface plasmon resonance, in which electrons on a surface are excited by the photons in light and then move parallel to the surface. This effect enhances the reporter signal by 100× and can help to quantify a variety of details within the sample3.
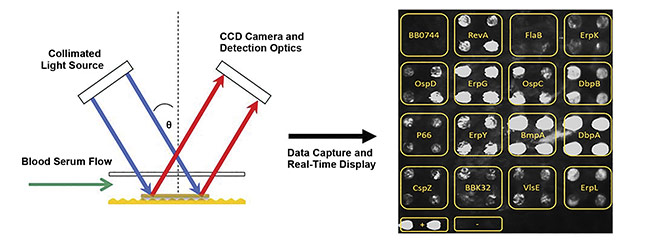
Figure 3. A schematic illustration of GC-FP analysis on the gold-coated biochip, using a fluorophore-labeled antibody to enhance the fluorescent signal (left) and a GC-FP image containing Lyme disease targets (right). Courtesy of Nathaniel Cady.
The researchers examined samples of 17 antigens from patients in various stages of the disease. They used blind sampling so that they did not know which category a particular serum fell into before the analysis was conducted. Their research showed that the assay platform could detect antibodies with a serum sample of 5 µl, with both specificity of 100% and sensitivity of 90%3.
“We looked at other technologies used to detect Lyme and compared our data with the two-tiered test,” said Arturo Pilar, president of Ciencia. “At some points, it’s at least as good at detecting Lyme, but our test is better in the early stages.”
He said the fluorescence was measured for 15 s exposure, though the time varied based on factors such as an overall low signal. The chip (Figure 4) was placed into a machine that reads the results. The Lyme-specific fluorescent signal was determined by subtracting the background signal and dividing it by the mean negative control spot signal. In the future, he said, this method may help to determine whether or not to treat a patient with antibiotics, and it could simplify post-treatment testing.
Figure 4. Student Eunice Chou applies fluid to the GC-FP biochip for analysis. Courtesy of
Melissa P. Renzi.
Both Cady and Pilar said they are seeking funding from agencies such as the National Institutes of Health to conduct tests on a larger sample size, from a broader geographic area across the nation. Cady said that, for the purposes of scientific and statistical analysis, it was important to test in areas that had already experienced a significant number of cases of Lyme disease, so that the researchers could be certain that samples were being categorized properly, such as treated versus untreated cases.
The ultimate goal is to get approval for their diagnostic technology from the FDA. Cady said that, so far, the good results they have achieved foretell promise in the examination and diagnosis of other diseases.
“As long as you know what biomarkers you’re looking for, you can really apply this assay to any disease, including COVID-19, so the technology is agnostic,” he said.
Darkening effects of Lyme
Meanwhile, a research team from institutions in New York, Tennessee, Massachusetts, Maryland, and Oregon set out to create its own microfluidic serologic test for point-of-care diagnosis of Lyme disease via the use of silver and gold nanoparticles. When the silver nitrate and reducing agents are flowed through the chip, the silver ions undergo reduction and the detection zone darkens (measured by a photodiode) as a result of the presence of certain elements. The preliminary study also showed results that were superior to those of the standard two-tiered test advocated by the CDC.
The team gathered serum samples from patients with acute and convalescent early Lyme disease, Lyme arthritis, and post-treatment Lyme disease syndrome, as well as a control group. For the analysis, it chose three antigens associated with Lyme bacteria, along with a synthetic peptide (PepVF), to use in the microfluidic assay (contained within a cassette assembled by OPKO Health) (Figure 5) to determine sensitivity at various times in the disease’s progression. Sensitivity ranged from 80% to 100%, depending on the stage of the disease4.
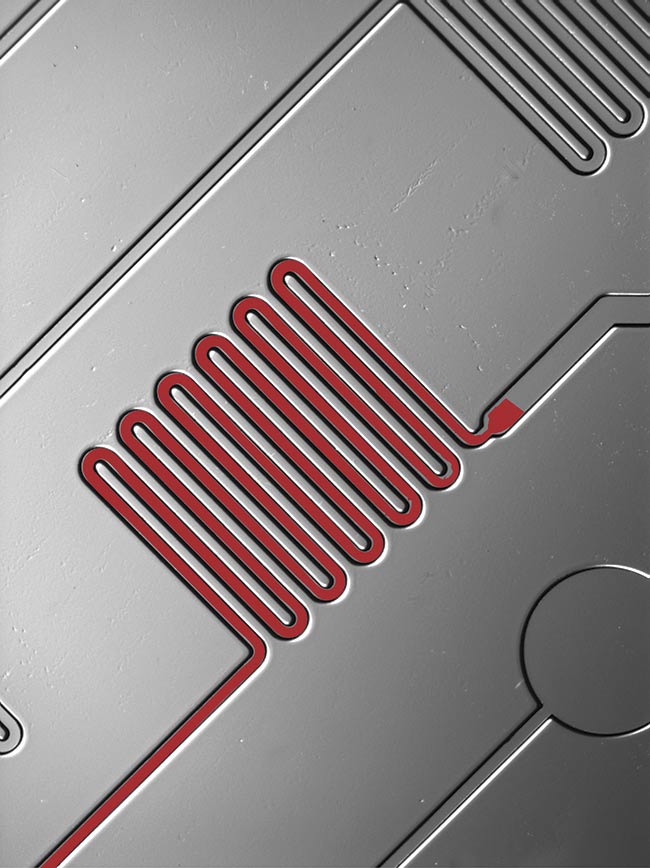
Figure 5. A close-up of fluid moving through a channel in a microfluidic chip designed to test for Lyme disease. Courtesy of Sia Lab/Columbia Engineering/OPKO Health.
“In our study, we were looking at absorbance as opposed to fluorescence, because as more proteins become apparent, the light from the silver nanoparticles that bind with them is reduced after it is hit with an LED and absorbed by our photodiode,” said Siddarth Arumugam, a doctoral candidate who works in the lab of Samuel Sia at Columbia University. “So we were looking at the optical density value in five detection zones that our microfluidic chip was designed for.”
Arumugam said the studies completed so far represent the proof of concept of their work, and they are seeking grant applications to test a far larger sample size in conjunction with the industry partners that are helping them produce the chips. So far, though, he said the assay can detect both early and late stages of the disease effectively, even though the antibody expression of Lyme changes over time.
Much like the chips from the SUNY collaboration, the serodiagnostic test could be used for a variety of diseases and conditions, Arumugam said.
“The platform itself is really agnostic,” he said. “We have done the same thing with the Zika virus. As long as you have [the] biomarkers you are looking for and have the necessary capture antibodies or proteins, you can optimize it for any application. In the future, we envision the potential of a clinician having different cassettes set up for different conditions that can easily be analyzed.”
Calls for testing grow
To work toward acceptance of their modality and for distribution on a broad scale, Arumugam said he and other researchers would work with a commercial partner to test a broader range of the population.
“Based on the commercial partner’s interest, we would work with them on doing a larger study using a wider variety of samples to demonstrate the consistency of our approach,” he said. “This would involve testing samples from patients with other tick-borne infections, and just a much larger cohort in general.”
Whatever analytical methodologies are brought forward for commercialization, they will be of great interest to hospital personnel, but also to public and private laboratories and physicians’ offices.
In its second report to Congress last year, the Tick-Borne Disease Working Group indicated that tick-borne illnesses, and Lyme disease in particular, were underreported nationally, with potential infection being 8 to 12× higher than officially diagnosed. The report stressed the need for the development of point-of-care diagnostic tests that would result in timely treatment of the disease.
The working group urged Congress and the National Institutes of Health to support new diagnostic technologies that identify specific aspects of the bacteria in Lyme disease and show not only that a person is infected, but at what stage the disease is in their system.
“The existing gaps in Lyme disease diagnosis underscore the critical need for the development of Lyme disease-specific diagnostics to enable health care providers to make an accurate diagnosis,” the group wrote in its report5. “Targeted funding in support of the development of such tests will result in marked improvement of patient care.”
References
1. A. Moore et al. (2016). Current guidelines, common clinical pitfalls, and future directors for laboratory diagnosis of Lyme disease, United States. Emerging Infect Dis, Vol. 22, Issue 7, pp. 1169-1177.
2. H. Joung et al. (2019). Point-of-care serodiagnostic test for early-stage Lyme disease using a multiplexed paper-based immunoassay and machine learning. ACS Nano,
Vol. 14, Issue 1, pp. 229-240.
3. E. Chou et al. (2020). A fluorescent plasmonic biochip assay for multiplex screening of diagnostic serum antibody targets in human Lyme disease. PLoS One, Vol. 15,
Issue 2, p. e0228772.
4. S. Arumugam et al. (2019). A multiplexed serologic test for diagnosis of Lyme disease for point-of-care use. J Clin Microbiol,
Vol. 47, Issue 12, p. e01142-19.
5. Tick-Borne Disease Working Group (2020). Report to Congress.
Testing Wearable Sensors
When flying to Norway a few years ago, Michael Snyder, a professor of genetics at Stanford University, was, in effect, a human guinea pig wearing numerous sensor technologies, including a smartwatch, a radiation monitor, and various types of oximeters. The devices gathered data on heart rate, blood oxygen level, skin temperature, activity level, and exposure to radiation.
Oximeters were placed on the forehead and finger, and Snyder said the latter produced the more reliable data.
He was one of ~60 people who agreed to wear the technology for two years. This particular flight was different, though. “My blood oxygen level was much lower than usual and my heart rate was also elevated,” he said. “That was my first indication something was not right.”

Stanford University professor Michael Snyder displays some of the wearable technologies he has been using to monitor his health, some of which helped him to detect Lyme disease at an early stage. Courtesy of Steve Fisch Photography/
Stanford Medicine.
He considered that Lyme disease might be the culprit: In recent weeks, he had been building a fence in a rural area in Massachusetts. Eventually, he noticed a fever. Blood tests later confirmed that he had contracted Lyme disease.
The wearable sensors helped identify the underlying condition before a number of other symptoms appeared.
“I always measure myself a lot on airline flights,” Snyder said. “Also, it is a time when SpO2 [oxygen saturation] normally drops. It was extra low during the Lyme case.”
While the researchers involved in the study acknowledged the possibility that wearables could lead to false alarms, the devices could also be personalized for each individual.
Other research that Snyder and his team have been involved in includes exploring the possibility of using wearables to detect diabetes, and more recently, using smartwatch data to detect symptoms such as heart rate elevation and changes in sleep patterns associated with COVID-19. The Stanford Healthcare Innovation Lab is currently seeking participants for a study analyzing the effectiveness of wearables in the early detection of COVID-19. For more information, visit
www.innovations.stanford.edu/wearables.